Transcript
Here's a pdf version of this transcript<--
Hello. Thank you, guys, for showing up again today. We took a couple of weeks off from our review of the female orgasm system. And now, we are ready to roll again.
Even Medical School Does Not Teach all of the Anatomy of the Female, and that Matters
When I was a kid, I remember wondering, "What the heck does the vagina look like?"
And then, as I got older and had girlfriends and then went to medical school and learned what the vagina is like, I was somewhat disappointed to realize that often it is thought about as if it were just a simple birth canal and a urinary tract and the elegance of the parts were not really discussed.
It turns out, my disappointment was not misplaced. An article that came out this year in the Journal of Sexual Medicine made a big point of the fact that not knowing about the female genital anatomy is not insignificant (Peters, 2023); if we don't think about the parts—all of the parts—then we do not know best how to treat dysfunction.
Another article demonstrated that, of seven medical schools in the Chicago area, only one was teaching all of the components of the clitoris (Codispoti, 2023). And the irony is that, in that article, they did not even test for all the parts. They left one of the components of the anatomy, the clitoral root, out of their evaluation of the curriculum.1
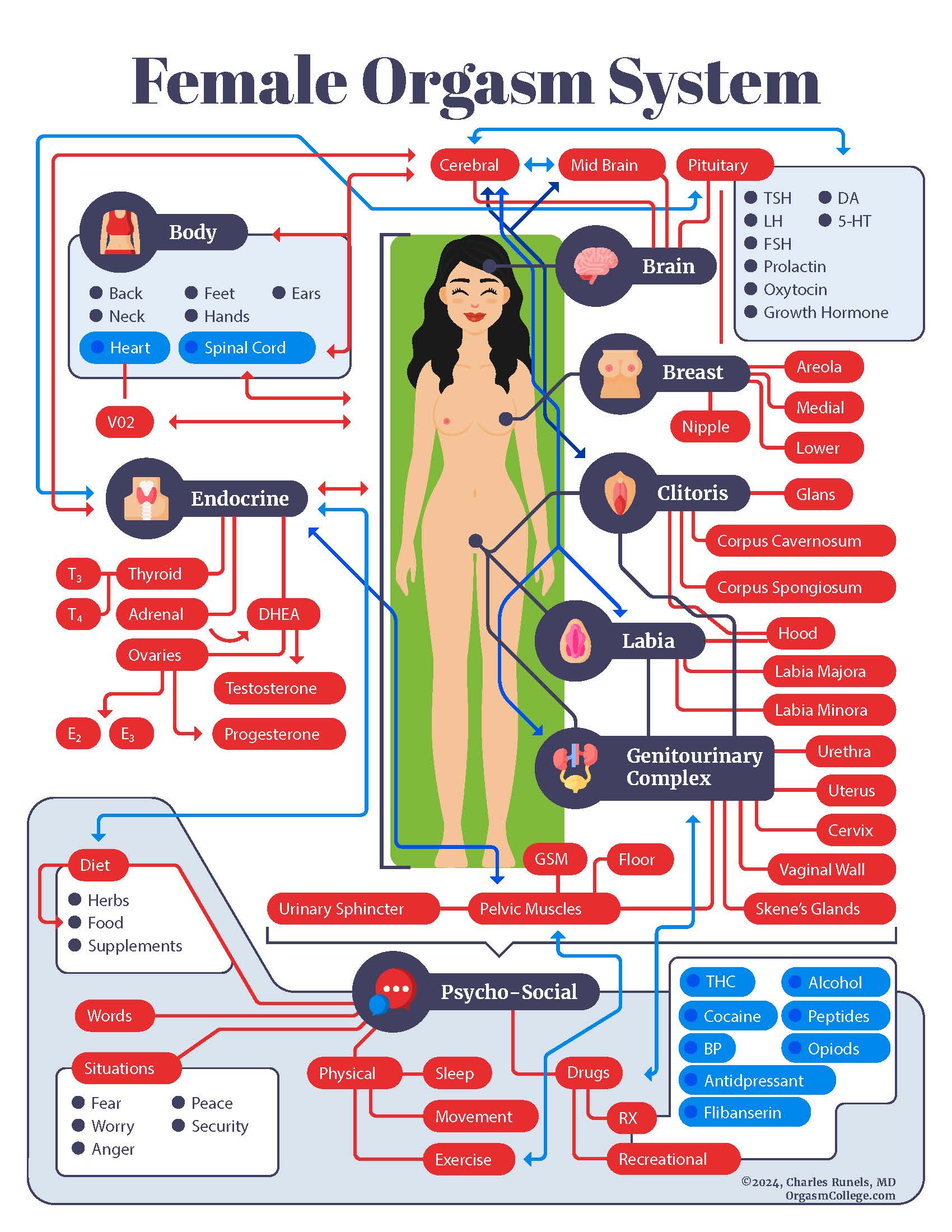
What is the “Female Orgasm System”?
There are two components of the female orgasm system that I think are most nebulous. Not only are they unseen, they are less discussed and more vaguely conceptualized by most physicians. Before we think about them, take 30 seconds to review what we were doing with this series of lessons: a systems analysis of the female orgasm.
Systems analysis first involves, "What's the purpose of all the parts working together?"
There is overlap; some parts work in both the respiratory and cardiovascular systems. Some parts of the urinary system are in the reproductive system or in the orgasm system. But, when you have a discreet set of parts that perform a specific function (in this case, sexual arousal in females, not reproduction, but sexual arousal, sometimes leading to orgasm)—then that is a separate system.
You can become more and more detailed by dividing each component, each subcomponent, and each sub-sub-component going on for infinity into the sub-particle level and eventually into ethics, philosophy, and mathematics (since everything is related to everything). But, clinically and practically, first-order components are most important to help women to better health and marriages.
You cannot really think about how all the parts work together if you do not even think about “What are all the parts?”
Two Nebulous Parts of the Female Orgasm System
An article showed that (looking at medical schools) not all the parts are even being taught. I made a sketch (see the video) from a detailed article showing the suspensory ligament, prepuce (the hood), body, and glans. In the sketch, you will also see the root and the bulb; these two components of the female orgasm system seem nebulous to most people.
The Bulb of the Clitoris
At one time, the bulb was considered part of the labia, but it is contiguous with the body of the clitoris. And so, most people consider it, now, to be equivalent to the corpus spongiosum of a male and as just as much a part of the clitoris as the corpus spongiosum is to the penis.
More about the bulbs later.
The Root of the Clitoris
But the root is even more nebulous. Let me show you something that I did this morning. I think this will shock you: I went to the AI app that everybody's using now. When you search for the “root of the clitoris” in the new AI application, it says, "The clitoris is a complex organ, highly sensitive organ, female genitalia. It doesn't have a root like a plant does. Instead, it has a visible and internal components,"
I will show you how the root relates to the G-spot, the urethra, and sexual function. Before I do, consider the root from the lover’s perspective (including the woman who loves herself (I am only partly referring to masturbation).
Why the Root Matters in the Lover’s Mind
I have a friend, Anne Kent Rush, who co-authored and illustrated the first massage book published in the United States that was written for people other than physical therapists (Downing, 1972). I first read it when I was about 17, and I’m 63 right now.
Back in the '50s, massage therapists were thought to be people who gave you a happy ending, and their places of business were in the red-light districts. But, Ms. Rush, with her writing did much to change that.
In her book (co-authored with Downing), she gave what I think to be great advice for lovers or massage therapists. She said, "Let your hands talk to the other person about their own body."
So, if you are touching someone's back and you're just rubbing it absent-minded like their back is a piece of meat, that's one thing. But if you can actually see (in your mind’s eye) and say to the person, “Here are your splenius capitis; here are your paraspinal muscles; here is your trapezius; and here are the insertion sites, and here is the full length and beauty of this muscle,” and your hands are gently teaching the person, showing the person, the individual muscles and how miraculous their body-temple is constructed, then they are going to enjoy a beautiful massage.
How much more so if you do the same with the genitalia?
So, translate that idea over to lovemaking and imagine making love to your lover’s genitalia with full knowledge of all the seen and the unseen.
Now imagine the opposite: I have seen very bright physicians come to my workshops, and when we do the hands-on practice of how to do the O-Shot® procedure, and their wife is the model, I am often shocked to see the spouse fumble with the identification of the anatomy while doing a procedure on his own wife. And, I guess I shouldn't be shocked since we just discussed that female genital anatomy is not taught in medical school; so where was he to learn it? From the football coach who taught him sex education in high school?
If you are going to be the doctor to people with vaginas or you are going to be the lover of people with vaginas, even whether the vagina is yours or another person's, it might be helpful to know all the parts so you can love on them or treat them, whatever the case may be.
I acknowledge that, in the heat of passion with the woman you love, no one thinks about the intricacies of the clitoral anatomy. In the heat of passion, it is just sweat and sounds, and no one is speaking like the Oxford English Dictionary or thinking about the intricate connections of the prepuce or the suspensory ligament; that’s not happening.
But, on the other side of that, knowing every part could make you a better lover and it could certainly make you a better physician. Maybe I am overemphasizing the point, but I don't want you to think that I think it is necessary to know every part, to have good love-making, I think it can take things to another level if combined with the rest of your passion and intellect.
I sketched my version of it, a simplified version of the root (see the video). Part of the confusion for the confusion regarding the root is that the multiple planes of the crus and the bulbs make it difficult to illustrate. But, if you look at this dorsal view, you can see the glans, the body, and the clitoris. It comes down to this area, from which the corpus splits away. And it's been dissected, where you can see it on the patient's left, but not on the right (refer to the video).
And then, if you look at the transverse view, you can see one of the corpus cavernosi, coming towards you, and you can see the suspensory ligament. And, as you know, there's another corpus cavernosi going away from you.
So, let me draw it, in just about as simple as I could draw it, which would be like this. Here's glans, and here's corpus cavernosi. But what do you call that? That is not the glans, it's not the body, it's not the corpus cavernosi, it's the root.
In spite of what your artificial intelligence app says. The clitoris does have a root. It is talked about in the research; it is important; and you should know what it is and where it is.
Do we want to just go back to thinking of the introitus, labia, and clitoris as just a glob of tissue, or do we actually want to understand it?
Of course, you do because you're on this call!
Here’s a crucial point from one of my favorite papers regarding female anatomy (Pauls, 2015), discussing the clitoral root,
"It's positioned beneath the skin of the vestibule and forms the connection from the clitoral body to the crura, overlapping with the two bulbs of the vestibule. The root is considered of importance because of the sensation. The convergence of the clitoral erectile bodies may be the most responsive to direct stimulation, owing to its superficial location and its depth of erectile tissue."
Okay? Read that again and tell me the root is not important. I dare you.
Dr. G, the G-Spot, and the Clitoral Root
Now, think about where the root is:
The urethral orifice lies at the most posterior portion of the clitoral root. So, if you go back to this picture, the clitoris is angling down (caudal). And the urethral orifice is near the root.
Now, think about what the G-spot is:
Dr. Grafenberg's big idea was not really regarding a spot. His noticing was that pressure on the urethra, not a spot, the urethra, was the most stimulatory thing possible to a woman’s body. Pressure there resulted in the most amazing orgasms. And he documented or described female ejaculation from stimulating the urethra with pressure on the anterior vaginal wall (Grafenberg, 1950).
Pressure from the anterior vaginal wall against the urethra, the root is right there. The root is very responsive to stimulation (Oakley, 2013). It could be that part of what's happening when you stimulate the so-called G-spot2: pressure there is definitely going also to stimulate the clitoral root.
So, when Dr. Grafenberg described stimulation of the urethra, he was also stimulating the clitoral root.
Corollaries of Acknowledgment of the Clitoral Root
Considering the clitoral root, "What can go wrong?"
Vaginal delivery can tear the area. One of our gynecologists told me that when she delivers the babies of women who suffer genital mutilation, the whole clitoral body can be torn, including the root. It sometimes must be sutured back together postpartum.
Perhaps knowing about the root, should you wish for self-pleasure or pleasuring your lover, knowing that it's not just the vagina and the urethra that matters, but there's a root to the clitoris, from which the corpora and the body originate, like a root, branches coming off of a root. Then, that understanding could make things better.
When Bruce Lee discussed martial arts in his book on fighting (Lee, 2018), he said that after you study the book and learn it, you tear it up and throw it away. When fighting, the individual methods and specific learning go out the window the first time someone hits you in the nose. But, in the art and in instinct that guides the fists will be embedded, the learning from the book discarded. And so it is with lovemaking. You learn the anatomy and then forget the anatomy in the bedroom; still, things could be better with your eyes closed because of what you learned when they were open.
The sensitivity of the clitoral root also explains why size might matter—not big or little or loose or tight, but the best fit between one man and one woman will put pressure on the root—but not too much.
Moreover, assuming that there's something other than penis and vagina sex, knowing and understanding the clitoral root can make a difference to what one might be doing with hands and tongue; back to my analogy, with massage. If you know what's there, and you talk to your lover with your hands and tongue about what you are discovering, that can be much different than if you are only manipulating a big “glob of stuff” you don’t understand.
Disclaimer
Just to avoid as many arrows as possible, with every lesson, I like to remind you that I understand there is much more to a woman than her vagina—that’s the whole point of what we are doing: there is a system, there's the psychology, the sociology, the hormonal milieu, the circulation, so many other things, but why not understand all the parts? And back to the irony, this part (the root) was not included in the test of the medical school curriculum—the testers omitted one of the parts of the system about which they were testing.
To summarize the root:
The root is the intersection of the two corpus cavernosum, the body of the clitoris and the bulbs of the clitoris. It lies above the urethra. It's very responsive to stimulation. And we should know what it is and where it is.
More about the Bulbs
Now, back to the bulbs.
The bulbs are, let's go back to this picture (see the video); the bulbs are up to seven centimeters long. The bulb, look at it, it lies just along the edge of the labia minora and is contiguous with the body and the glans clitoris, and fills that space with tissue that is also both erectile and trabecular.
A lesson from the penis
Reconsider men for a moment. By the time a man reaches 65, he loses about 50% of the endothelium. With women, Delancey and others have documented that the nerves and muscles of the clitoris and urethra atrophy; in his cadaver studies (see multiple references listed below).
Further, we know that platelet-rich plasma causes neurogenesis and angiogenesis (see references). When we do our O-Shot® procedure, we're injecting the body of the clitoris, which is connected to the root, the crura, and the corpus spongiosum, or the bulb. As expected, after this injection, a woman’s sex can improve dramatically. (See representative references regarding the O-Shot® procedure here<—).
This cutaway view (see video), I think, is also very illuminating. I love this paper. And because you can see they're holding the body of the clitoris. They've cut away just along the edge of the labia minora. And you can see the bulb or the corpus spongiosum, right there, lying underneath the mound of the labia majora. Now, the tissue of the labia majora, so it's lying above.
Let's go back and look at this picture. Here is the introitus. So, it stops beneath the urethra, near Bartholin's gland, at the upper part of the introitus.
So, looking back here, it would go down, beneath the urethra, and it would come over, lying beneath the mound of the labia majora. And, remember, it's erectile and has sensation.
Now, when we do our O-Shot, we are injecting the body of the clitoris. When we do the Vampire Wing Lift® procedure, we inject PRP into the anterior half of the labia majora. And I don't propose that we are always accurately inserting that needle in the center of the corpus spongiosum. But there's enough volume there that there would definitely be a field effect that improves the function of the bulbs.
When you treat the hair, you don't have to cover every millimeter. If you're within a centimeter of an area, you are going to affect hair growth. And, oftentimes, you'll even see improvement in the skin of the forehead because there's a field effect. Platelet-rich plasma recruits pluripotent stem cells that migrate to the area and propagate regeneration of healthy tissue, collagen, nerve, and blood flow. And it's not just where the lumen of your needle happens to be exactly within a millimeter of the area intended.
So, I think I'm okay with being more lucky than smart. My original idea of doing the Vampire Wing Lift® procedure was injecting and restoring volume and rubor, like we do with the Vampire Facelift® procedure. I didn't really contemplate the idea that, in all likelihood, we're also improving the sensation and function and restoring some of the volume of the bulb or the corpus spongiosum.
So, the bulb lies in a triangular space of three to seven centimeters. It probably provides some structure that improves sensation with sexual intercourse.
"The bulb or homologous corpus spongiosum, they engorge during arousal, some lubrication function, but also conferring stability on the vaginal walls."
So by this explanation, the bulbs bring the clitoral tissue closer to the vaginal lumen during arousal.
Remember, we looked at a cross-section of the penis within the vagina, and we contemplated the following: “Without structure, there is no pressure."
The penis, without the structure supporting the vaginal walls, would have no pressure against the urethra, the root, the corpus cavernosi, the corpus spongiosum, or the bulb.
Conclusion
The more I read, the more I realize the vastness of what I don't know—even after reading all that I can read. There is much to know and even more to discover.
One year ago, I couldn't have given you a good explanation of what the root of the clitoris is. And now that I know, I have more questions than answers.
I say this to restate that what we're doing here is worth doing. Pointing out, if medical schools don't even teach all the parts of the clitoris, then, I think this project we're doing, defining the Female Orgasm System (it’s parts and how they work together) is worth doing.
I’m so very grateful that you're showing up for these webinars because it motivates me not to stop; it means that maybe at least somebody's interested. And there appears to be quite a few of you guys that are interested. Hope you'll spread the word. I'm not charging for any of this. I'm just putting it out, editing it some, before I put it out, with the mission that people realize that it's not just a glob of stuff down there.
And just knowing the parts doesn't fix anything.
I spoke with a very prominent gynecologist/pelvic reconstructive surgeon, and he proceeded to explain to me all the parts. And I was thinking, "Yep. Know it. Know it. Know it." But, knowing all the parts would be like lifting the hood of your car, but that doesn't mean you know how they're functioning together, as a system, to make your car go down the road."
So, we have, first, I think, to label all the components.
Then, there's this idea: “How are they working together?"
We haven't even gotten to the other parts, like the pelvic floor muscles. "How do they work together to help both with continence and improvement in sexual function?"
And, "How do they work together, with the clitoris and all the rest of the system, to create pleasure?"
But I think that's all I have today. Hopefully, that's helpful. And, hopefully, next time somebody asks you about the parts of the clitoris, you'll know exactly about the root and the bulb.
Have a great day. Goodbye.
References
- Codispoti N, Negris O, Myers MC, et al. Female sexual medicine: an assessment of medical school curricula in a major United States city. Sexual Medicine. 2023;11(4):qfad051. doi:10.1093/sexmed/qfad051
- DeLancey JOL, Trowbridge ER, Miller JM, et al. Stress Urinary Incontinence: Relative Importance of Urethral Support and Urethral Closure Pressure. J Urol. 2008;179(6):2286-2290. doi:10.1016/j.juro.2008.01.098
- DeLancey JO. Structural aspects of the extrinsic continence mechanism. Obstet Gynecol. 1988;72(3 Pt 1):296-301.
- DeLancey JO. Structural support of the urethra as it relates to stress urinary incontinence: the hammock hypothesis. Am J Obstet Gynecol. 1994;170(6):1713-1720; discussion 1720-1723. doi:10.1016/s0002-9378(94)70346-9
- Downing G. The Massage Book. 25th anniversary ed. Random House : The Bookworks; 1998 (first published 1972)
- GRÄFENBERG, Ernest (1950) The role of urethra in female orgasm, in: The International Journal of Sexology vol. III, no. 3: 145-148.
- Lee B. Tao of Jeet Kune Do. Expanded ed. Black Belt Books; 2018.
- Oakley SH, Mutema GK, Crisp CC, et al. Innervation and Histology of the Clitoral–Urethal Complex: A Cross-Sectional Cadaver Study. The Journal of Sexual Medicine. 2013;10(9):2211-2218. doi:10.1111/jsm.12230
- PANDIT M, DELANCEY JOL, ASHTON-MILLER JA, IYENGAR J, BLAIVAS M, PERUCCHINI D. Quantification of Intramuscular Nerves Within the Female Striated Urogenital Sphincter Muscle. Obstet Gynecol. 2000;95(6 Pt 1):797-800. Accessed October 20, 2021. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1192577/
- Perucchini D, DeLancey JO, Ashton-Miller JA, Peschers U, Kataria T. Age effects on urethral striated muscle I. changes in number and diameter of striated muscle fibers in the ventral urethra. American Journal of Obstetrics & Gynecology. 2002;186(3):351-355. doi:10.1067/mob.2002.121089
- Perucchini D, DeLancey JOL, Ashton-Miller JA, Galecki A, Schaer GN. Age effects on urethral striated muscle II. Anatomic location of muscle loss. American Journal of Obstetrics and Gynecology. 2002;186(3):356-360. doi:10.1067/mob.2002.121090
- Pauls RN. Anatomy of the clitoris and the female sexual response. Clinical Anatomy. 2015;28(3):376-384. doi:10.1002/ca.22524
- Peters B, Ndumele A, Uloko MI. Clinical implications of the historical, medical, and social neglect of the clitoris. J Sex Med. 2023;20(4):418-421. doi:10.1093/jsxmed/qdac044
References-PRP for Neurogenesis
- Wu YN, Liao CH, Chen KC, Chiang HS. Dual effect of chitosan activated platelet rich plasma (cPRP) improved erectile function after cavernous nerve injury. Journal of the Formosan Medical Association. Published online March 27, 2021. doi:10.1016/j.jfma.2021.01.019
- Yasak T, Özkaya Ö, Ergan Şahin A, Çolak Ö. Electromyographic and Clinical Investigation of the Effect of Platelet-Rich Plasma on Peripheral Nerve Regeneration in Patients with Diabetes after Surgery for Carpal Tunnel Syndrome. Arch Plast Surg. 2022;49(02):200-206. doi:10.1055/s-0042-1744410
- Foy CA, Micheo WF, Kuffler DP. Functional Recovery following Repair of Long Nerve Gaps in Senior Patient 2.6 Years Posttrauma. Plast Reconstr Surg Glob Open. 2021;9(9):e3831. doi:10.1097/GOX.0000000000003831
- Kuffler DP. Platelet-Rich Plasma and the Elimination of Neuropathic Pain. Mol Neurobiol. 2013;48(2):315-332. doi:10.1007/s12035-013-8494-7
- Sánchez M, Anitua E, Delgado D, et al. Platelet-rich plasma, a source of autologous growth factors and biomimetic scaffold for peripheral nerve regeneration. Expert Opinion on Biological Therapy. 2017;17(2):197-212. doi:10.1080/14712598.2017.1259409
- Chung E. Regenerative technology to restore and preserve erectile function in men following prostate cancer treatment: evidence for penile rehabilitation in the context of prostate cancer survivorship. Therapeutic Advances in Urology. 2021;13:17562872211026421. doi:10.1177/17562872211026421
- Pandunugrahadi M, Irianto KA, Sindrawati O. The Optimal Timing of Platelet-Rich Plasma (PRP) Injection for Nerve Lesion Recovery: A Preliminary Study. Int J Biomater. 2022;2022:9601547. doi:10.1155/2022/9601547
- Abo El Naga HA, El Zaiat RS, Hamdan AM. The potential therapeutic effect of platelet-rich plasma in the treatment of post-COVID-19 parosmia. The Egyptian Journal of Otolaryngology. 2022;38(1):130. doi:10.1186/s43163-022-00320-z
- Aaraj MA, Boorinie M, Salfity L, Eweiss A. The use of Platelet rich Plasma in COVID-19 Induced Olfactory Dysfunction: Systematic Review. Indian J Otolaryngol Head Neck Surg. Published online June 10, 2023. doi:10.1007/s12070-023-03938-4
References PRP for Neovascularization
- Bindal P, Gnanasegaran N, Bindal U, et al. Angiogenic effect of platelet-rich concentrates on dental pulp stem cells in inflamed microenvironment. Clin Oral Investig. 2019;23(10):3821-3831. doi:10.1007/s00784-019-02811-5
- Miłek T, Nagraba Ł, Mitek T, et al. Autologous Platelet-Rich Plasma Reduces Healing Time of Chronic Venous Leg Ulcers: A Prospective Observational Study. In: Pokorski M, ed. Advances in Biomedicine. Advances in Experimental Medicine and Biology. Springer International Publishing; 2019:109-117. doi:10.1007/55842019388
- Norooznezhad AH. Decreased Pain in Patients Undergoing Pilonidal Sinus Surgery Treated with Platelet-Rich Plasma Therapy: The Role of Angiogenesis. Advances in Skin & Wound Care. 2020;33(1):8. doi:10.1097/01.ASW.0000615376.97232.0a
- Li Y, Mou S, Xiao P, et al. Delayed two steps PRP injection strategy for the improvement of fat graft survival with superior angiogenesis. Sci Rep. 2020;10:5231. doi:10.1038/s41598-020-61891-6
- Zhang XL, Shi KQ, Jia PT, et al. Effects of platelet-rich plasma on angiogenesis and osteogenesis-associated factors in rabbits with avascular necrosis of the femoral head. Eur Rev Med Pharmacol Sci. 2018;22(7):2143-2152. doi:10.26355/eurrev20180414748
- Nolan GS, Smith OJ, Heavey S, Jell G, Mosahebi A. Histological analysis of fat grafting with platelet‐rich plasma for diabetic foot ulcers—A randomised controlled trial. Int Wound J. 2021;19(2):389-398. doi:10.1111/iwj.13640
- Sclafani AP, McCormick SA. Induction of dermal collagenesis, angiogenesis, and adipogenesis in human skin by injection of platelet-rich fibrin matrix. Arch Facial Plast Surg. 2012;14(2):132-136. doi:10.1001/archfacial.2011.784
- Araujo-Gutierrez R, Van Eps JL, Scherba JC, et al. Platelet rich plasma concentration improves biologic mesh incorporation and decreases multinucleated giant cells in a dose dependent fashion. Journal of Tissue Engineering and Regenerative Medicine. 2021;15(11):1037-1046. doi:10.1002/term.3247
- Fernandez-Moure JS, Van Eps JL, Scherba JC, et al. Platelet-rich plasma enhances mechanical strength of strattice in rat model of ventral hernia repair. Journal of Tissue Engineering and Regenerative Medicine. 2021;15(7):634-647. doi:10.1002/term.3200
- Saputro ID, Rizaliyana S, Noverta DA. The effect of allogenic freeze-dried platelet-rich plasma in increasing the number of fibroblasts and neovascularization in wound healing. Ann Med Surg (Lond). 2022;73:103217. doi:10.1016/j.amsu.2021.103217
- The clitoral root is thought by some anatomist to be very important to sexual arousal (Pauls,2015); but it is often not mentioned in anatomical descriptions of the vagina. The current author, asked his favorite AI app about the clitoral root, and the AI denied the existence of any such anatomical part. ↩︎
- which I always choke on that, because I think it's not really a specific unmovable spot. I think it's just that part of that area, that happens to be most sensitive, at that particular moment, for that woman on that day. It may be different five minutes from now. ↩︎
Subscribe to this course for free<--